Innovative biotechnology leader developing transformative new drugs
NYRADA INC. (NYR.ASX)
Introduction. Nyrada Inc. (ASX:NYR) is a clinical-stage Australian biotechnology company developing small-molecule therapies targeting critical unmet needs in neuro- and cardioprotection. Its lead candidate, XolatrypTM, is a first-in-class Transient Receptor Potential Canonical (TRPC) ion channel inhibitor designed to mitigate secondary brain injury after stroke and traumatic brain injury (TBI). Additionally, Xolatryp reduces heart muscle damage and improves cardiac function following myocardial ischemia-reperfusion injury (MIRI) and associated arrhythmias.
Breakthrough Preclinical Success. In a recent preclinical coronary heart disease study, Xolatryp provided 42% cardioprotection and reduced ventricular arrhythmias by 88% after MIRI. Additionally, in a recent penetrating TBI study conducted in collaboration with the Walter Reed Army Institute of Research, Xolatryp provided a statistically significant (p = 0.043) neuroprotective effect following a penetrating TBI.
Successful Phase I Clinical Trial Cohort Dosage. NYR has completed the dosage of all 6 cohorts as part of the trial that aims to evaluate the safety and tolerability of Xolatryp. Notably, no safety signals, toxicities, or unexpected adverse events have been reported to date. A safety and pharmacokinetic review will be conducted by the SRC once all data is available, and a final clinical study report is expected to be completed in the coming months. NYR has also committed to starting a Phase IIa clinical trial in the first quarter of 2026.
A Promising Biotech Company Underappreciated by the Market. Xolatryp has demonstrated exceptional preclinical efficacy for neuro and cardioprotection in addition to a Phase I clinical trial nearing completion, positioning it as a potential first-in-class therapy addressing unmet medical needs. With upcoming clinical milestones expected to drive a stock revaluation, NYR’s current market cap of A$78.0m appears notably discounted, indicating significant upside potential.
Read our equity research report on Nyrada by clicking the Equity Research button below. For additional insights into why we believe Nyrada is the best risk–reward biotech on the ASX, click the Latest Report button below.
EQUITY RESEARCH LATEST REPORT
NYRADA INC WEBSITE

KEY INVESTMENT INSIGHTS
Clear Business Strategy
Nyrada is focused on drug discovery and developing innovative new treatments for which there is a large unmet clinical need and substantial market potential. The company aims to develop best-in-class drugs focusing on neuroprotection (TBI) and cardioprotection (MIRI). Nyrada’s lead drug candidate – Xolatryp – has demonstrated strong preclinical efficacy in protecting the brain from secondary injury following stroke, in addition to strong preclinical efficacy in protecting the heart following acute MIRI. The ability to leverage two applications from one drug candidate places Nyrada in a strong position to ensure commercial success via an economical and efficient pathway.
Nyrada has a well-defined strategy to maximise the value of its drug development pipeline through targeted out-licensing. Importantly, Nyrada’s business model allows for licensing agreements based on specific indications and geographic markets, creating a flexible and scalable path to commercialisation. By pursuing this approach, Nyrada can leverage partnerships with larger pharmaceutical companies to handle manufacturing and distribution, enabling a capital-efficient strategy to monetise its R&D investments while focusing on further innovation.
High Barriers To Entry
The high barriers to entry in the markets NYR is targeting are illustrated by the presence of only 3 other competitors in the neuroprotection market and none in the cardioprotection market. This scarcity of competing development programs likely reflects both the scientific complexity of the field and the innovative nature of NYR’s approach. The company’s advanced position in this nascent space could translate into significant first-mover advantages and potential market exclusivity, pending successful clinical development.
The success of recent preclinical studies, such as the 2024 stroke and coronary heart disease trials, further underscores the efficacy of Xolatryp in providing neuroprotection and cardioprotection. This expanding body of evidence enhances Nyrada’s intellectual property position by highlighting the distinctiveness and therapeutic potential of its compounds. Additionally, the nearly complete Phase I clinical trial is expected to yield further supportive data, which could form the basis for future patent applications.
During the first half of FY25, NYR submitted ‘Composition of Matter’ patent applications in key geographies, including Australia, Europe, and North America, to safeguard the chemical structure of its TRPC channel-blocking intellectual property. Once granted, these patents will ensure that NYR retains exclusive rights to its TRPC assets for at least 20 years from the submission date.
Expanding its patent portfolio in this manner will be critical to maintaining Nyrada’s competitive advantage and securing long-term commercial opportunities in these high-value therapeutic areas.
Successful Management
The Nyrada Board and management team include leading figures in biotech, both here in Australia and the US, who have a proven track record of success in commercialising innovative technology. Nyrada’s CEO, James Bonnar, a chemist by training, brings 25 years of broad professional experience in the biotech industry. He has worked in preclinical drug development, product manufacturing, regulatory affairs, and clinical-stage drug research, most recently for Neuren, overseeing the development of treatments for TBI and neurodevelopmental disorders.
The Nyrada Board is a diverse mix of successful international entrepreneurs and dealmakers with proven track records in the pharmaceutical industry. Christopher Cox was the Chief Commercial Officer for The Medicines Company which developed the cholesterol-lowering drug Inclisiran®, a program that was acquired by Novartis in late 2019 for US$9.7B. At the time, it was the largest ever acquisition of a company with a single drug in development. Chris has extensive industry contacts, and this is an obvious benefit for Nyrada.
Marcus Frampton is the CFO for the largest sovereign wealth fund in the US, the Alaska Permanent Fund, and has a proven record in identifying and backing successful biotech companies. Companies they have supported include Juno Pharmaceuticals, an Australian company focused on the supply of off-patent drugs to hospitals. Dr. Rüdiger Weseloh works in commercial development for Merck KGA in Germany so he has a lot of experience negotiating and securing deals with pharmaceutical companies.
Nyrada’s Scientific Advisory Board comprises some of the world’s most respected scientific thought leaders from Australia, the US, France, and Japan. The Chair of the board, Prof. Gary Housley, is the Chair in Physiology at the University of New South Wales Sydney (UNSW) and is a founding director of the Translational Neuroscience Facility and has over 30 years of experience. Prof. Junichi Nabekura and Dr. Jim Palmer bring expertise in cardiovascular, neuroscience, and drug discovery programs, respectively.
Significant Investment Upside
At a market capitalisation of just A$78.0m, NYR appears significantly undervalued relative to its clinical progress, having successfully advanced through Phase I cohort dosage and now positioned to initiate Phase IIa trials. Furthermore, the neuroprotection and cardioprotection markets represent substantial, unmet medical needs, as there are currently no FDA-approved drugs with proven efficacy in these therapeutic areas. This positions NYR as a potential first mover, offering a meaningful competitive advantage over the limited number of players in the space. As the company progresses through clinical milestones and demonstrates further proof of concept, we anticipate that investor sentiment will shift, driving a revaluation of NYR’s stock.
MYOCARDIAL ISCHEMIC REPERFUSION EXPLAINED
Overview
Myocardial ischemia-reperfusion injury (MIRI) occurs when blood flow is restored to the heart muscle after an ischemic event (e.g., myocardial infarction), paradoxically causing additional damage. While reperfusion is critical to salvage tissue, it triggers oxidative stress, inflammation, microvascular dysfunction, and electrical instability, exacerbating cardiac injury and increasing the risk of arrhythmias.
Pathophysiology
Myocardial ischemic reperfusion is driven by several mechanisms:
- Oxidative Stress: Rapid reintroduction of oxygen generates excessive reactive oxygen species (ROS), damaging cardiomyocytes and destabilising cardiac electrical activity.
- Inflammation: Neutrophil infiltration and cytokine release impair endothelial function, contributing to tissue damage.
- Calcium Overload & Mitochondrial Dysfunction: Dysregulated calcium levels trigger mitochondrial permeability transition pore (mPTP) opening, leading to cell death and promoting arrhythmias.
- Microvascular Dysfunction: The “no-reflow” phenomenon prevents effective tissue perfusion, worsening ischemia.
- Electrical Instability & Arrhythmias: Ischemia and reperfusion disrupt ion balances (e.g., potassium, calcium), creating re-entry circuits and ectopic foci. This can lead to life-threatening ventricular arrhythmias, such as ventricular tachycardia or fibrillation, particularly within hours of reperfusion.
Epidemiology and Unmet Medical Need
MIRI is a major complication following myocardial infarction, especially in patients undergoing procedures like PCI. It often leads to arrhythmias, which are a leading cause of sudden cardiac death after a heart attack. Despite medical advances, there are no FDA-approved drugs specifically for MIRI or its related arrhythmias; current treatments focus only on revascularisation and symptom management, highlighting a significant need for targeted therapies.

STROKE EXPLAINED
Overview
Stroke occurs when the blood supply to a part of the brain is interrupted or reduced, depriving brain tissue of oxygen and nutrients. This leads to the rapid death of brain cells and subsequent neurological impairment. There are two main types: ischemic (caused by a blockage) and hemorrhagic (caused by bleeding).
Pathophysiology
Ischemic stroke (87% of cases) occurs when a blood clot or embolus blocks brain blood flow. This triggers a cascade of damage, including energy failure, excitotoxicity, oxidative stress, inflammation, and cell death. Hemorrhagic stroke results from bleeding in or around the brain. Secondary brain injury processes play a significant role in the progression of damage after the initial injury. These include excitotoxicity, neuroinflammation, oxidative stress, and a compromised blood-brain barrier.
Epidemiology and Unmet Medical Need
Stroke is a leading cause of death and disability worldwide, with an estimated 15 million people experiencing a stroke annually. Of these, approximately 5 million die, and another 5 million are left permanently disabled. While treatments like thrombolytics and thrombectomy help in acute ischemic stroke, they are time-sensitive and benefit only a small subset of patients. No therapies target secondary brain injury, which continues after the initial stroke.
TRAUMATIC BRAIN INJURY EXPLAINED
Overview
Traumatic Brain Injury (TBI) is a complex medical condition caused by an external mechanical force that disrupts the normal functioning of the brain. TBI can result from various incidents, including falls, motor accidents, and sports injuries. The severity ranges from mild (concussion) to severe, with outcomes varying based on injury extent.
Pathophysiology of TBI
The primary injury occurs at impact, leading to contusions, lacerations, and diffuse axonal injury. Long-term damage is driven by secondary mechanisms, including:
- Excitotoxicity: Excessive release of excitatory neurotransmitters can result in neuronal cell death.
- Neuroinflammation: The brain’s immune response to trauma can exacerbate tissue damage.
- Oxidative Stress: The production of reactive oxygen species can damage cellular structures, including membranes, proteins, and DNA.
- Blood-Brain Barrier (BBB) Disruption: Trauma can compromise the integrity of the BBB, allowing harmful substances to infiltrate the brain and worsen inflammation.
- Ischemia and Hypoxia: Reduced blood flow and oxygen delivery to the brain can lead to further neuronal injury.
Epidemiology and Unmet Medical Need
TBI is a leading cause of death and disability, with millions of cases annually. According to the World Health Organisation, it’s expected to surpass other diseases as a major cause of death by 2030. Current treatment focuses on supportive care, with no FDA-approved drugs addressing TBI’s underlying mechanisms.
TRPC CHANNELS EXPLAINED
Overview
TRPC channels are activated in response to physiological stressors such as ischemia, inflammation, and excitotoxicity. When triggered, they allow calcium and other cations to enter the cell. This calcium influx acts as a powerful cellular switch, initiating a cascade of intracellular signals that regulate inflammation, programmed cell death, metabolism, and tissue repair. While a controlled calcium signal is essential for healthy cell function, excessive calcium influx, as commonly occurs during acute injury, can overwhelm the cell’s protective mechanisms and lead to irreversible damage.
Backed By Research
TRPC channels play a critical role in injury-induced cell death, as shown by preclinical studies. A 2016 study using triple knockout mice (lacking TRPC3, TRPC6, and TRPC7) found significantly reduced heart damage after ischemia-reperfusion injury, indicating TRPC channels mediate calcium-related cardiac injury. Similarly, a 2023 study showed that deleting TRPC channels in mice led to strong neuroprotection after brain injury by preventing harmful calcium influx, reducing lesion size and neuronal damage. These findings highlight TRPC channels as key contributors to tissue damage in both heart and brain injuries.
Relevance to Humans
Mouse studies are valuable for modelling acute injury and testing drug targets because key cellular processes, like calcium regulation and cell death, are similar in mice and humans. TRPC channels, in particular, have conserved structure and function across species, making the findings highly relevant for human applications.
Nyrada’s Drug Development Strategy
NYR’s lead drug candidate, Xolatryp, targets TRPC3/6/7 activity after injury to prevent harmful calcium overload while preserving normal cell signalling. This approach addresses a key driver of cell death across organ systems, with the potential to reduce secondary damage and improve neurological and cardiac outcomes. It is supported by a strong scientific foundation and has clear relevance to large, underserved markets in acute care.
CARDIOPROTECTION PROGRAM
Preclinical Coronary Heart Disease Study
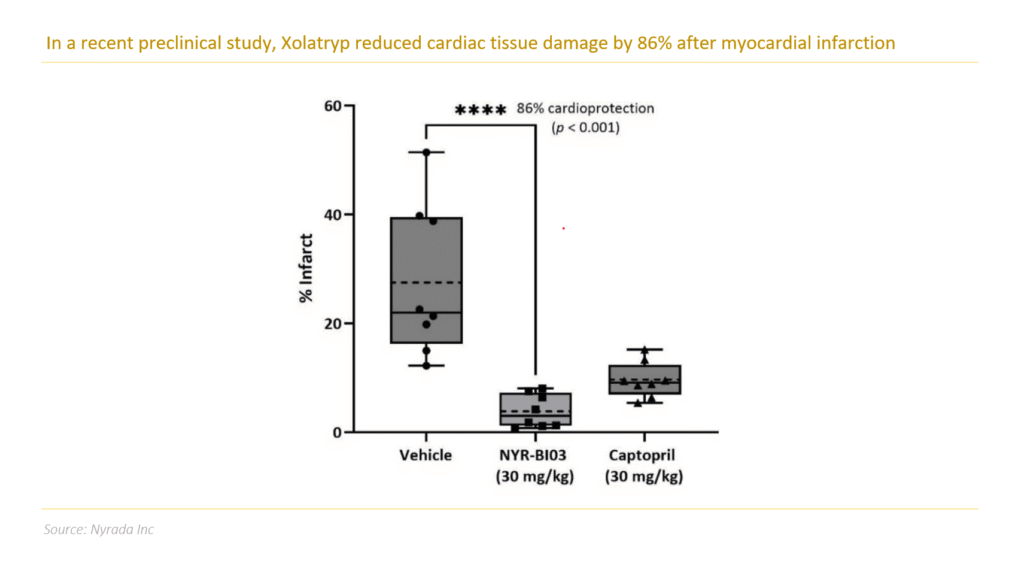
On 1 October 2024, NYR announced positive preclinical results for Xolatryp in MIRI. The preclinical rat study showed Xolatryp provided significant cardioprotection, reducing cardiac tissue damage by 86% (p < 0.001, n=8) following MIRI – a major cause of heart damage after blood flow restoration.
The study demonstrated Xolatryp’s strong efficacy in limiting cardiovascular damage following acute MIRI. Xolatryp notably outperformed captopril, an established FDA-approved ACE inhibitor traditionally used in managing post-ischemic events and used in the study as a positive control. By surpassing the performance of the current standard treatment, Xolatryp showcases promising potential as a novel therapeutic intervention for patients experiencing acute MIRI.
These preclinical results validate the drug candidate’s robust protective mechanisms and signal potentially significant therapeutic and commercial opportunities for NYR in the cardiovascular treatment landscape.
Supplementary Cardioprotection Preclinical Studies
On 23 October 2024, NYR announced supplementary results from its preclinical coronary heart disease study. The supplementary data confirmed that Xolatryp prevents loss of function resulting from MIRI following myocardial infarction (heart attack) in rats. In this supplementary data, Xolatryp delivered a substantial 43% increase in left ventricular ejection fraction (p < 0.0001), a key indicator of heart pumping ability, significantly improving overall cardiac function.
Currently, no FDA-approved therapies specifically target ischemia-reperfusion injury. The results further validate Xolatryp’s effectiveness in addressing ischemia-reperfusion injury related to heart attacks, enhancing the company’s potential to fill this critical treatment gap.
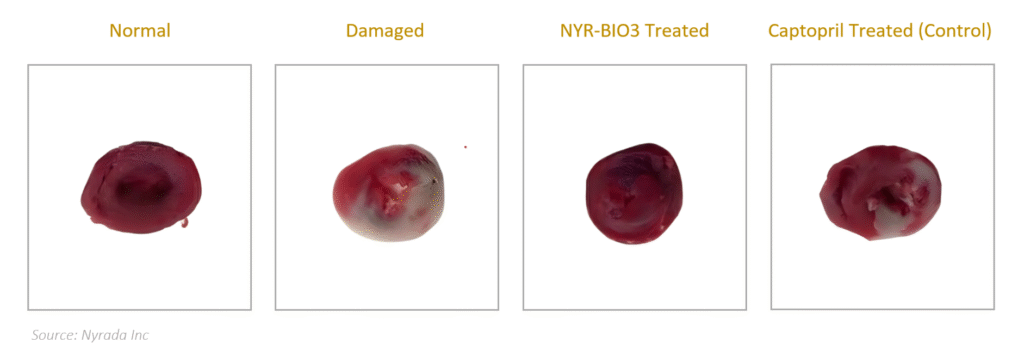
Rat Heart Sample Images
The images below depict sections of rat heart tissue from four groups: normal, damaged from ischemia-reperfusion, Xolatryp-treated, and Captopril-treated (current standard therapy) for visual comparison. Red-stained areas represent metabolically active tissue, while grey-stained areas indicate dead tissue. These images clearly demonstrate that damaged heart tissue treated with Xolatryp showed significantly better outcomes compared to both the control and Captopril-treated groups.
Preclinical Cardiac Arrhythmia Study
On 8 May 2025, Nyrada released results of a preclinical study in rats, which showed that the company’s Xolatryp drug provides strong cardioprotection when administered as a short-duration intravenous infusion following myocardial infarction (heart attack). The study showed that Xolatryp provided 42% cardioprotection when administered continuously for 3 hours. This latest study builds upon the company’s previous preclinical study in October 2024, and showed significant reductions in both heart muscle injury size and Troponin I, a key cardiac injury biomarker.
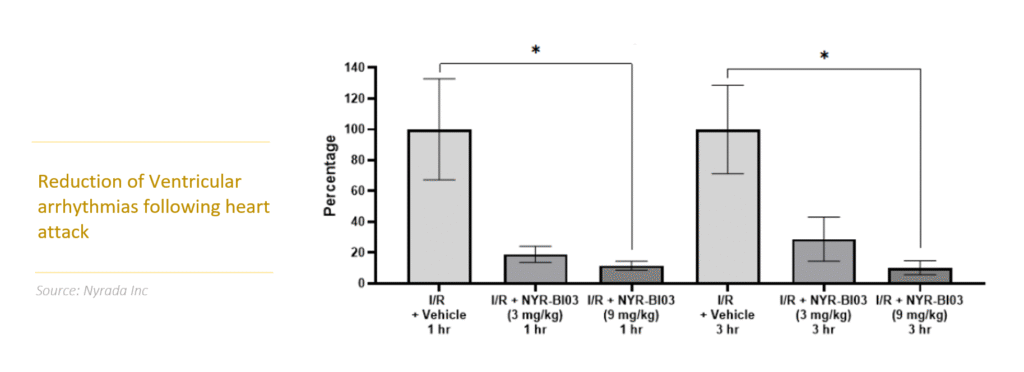
This study also showed that animals treated with Xolatryp had reduced incidence of ventricular arrhythmias (a condition where the heart beats at an irregular or abnormal rate, too fast, too slow, or with an irregular rhythm), which is a leading cause of sudden cardiac death following a heart attack. Animals treated with Xolatryp had an 88% reduction in ventricular arrhythmias at 1 hour and a 90% reduction at 3 hours (p = 0.04 at 1 hour and p = 0.01 at 3 hours, less than 0.05 is statistically significant).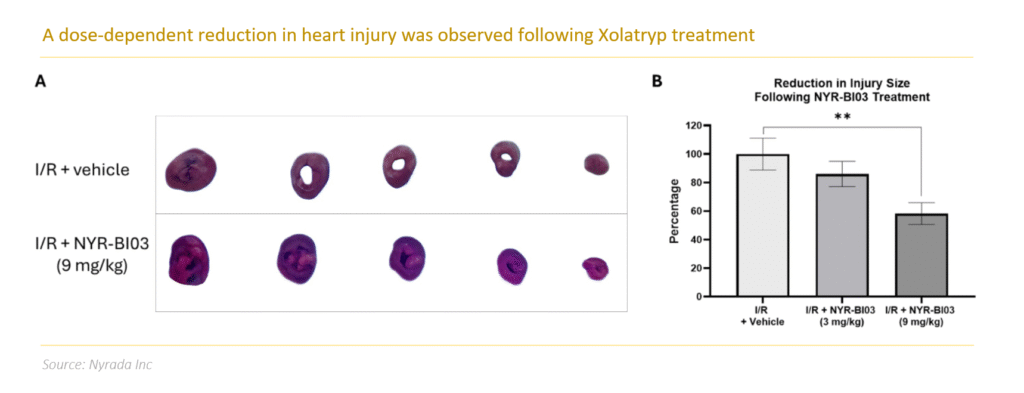
The study utilised the same rodent model from the October 2024 study, but the animals were administered at doses of 9.0 mg/kg of Xolatryp over 3 hours following acute myocardial ischemia (occurs when the heart muscle doesn’t get enough blood and oxygen due to restricted blood flow which can lead to a heart attack). Cardioprotection was confirmed with a short duration treatment compared with vehicle (placebo) with a 42% reduction in tissue death following heart attack (p = 0.008, less than 0.05 is statistically significant). This result is highly significant because it shows that the drug works over a shorter time period compared to the previous study, which involved administration over 24 hours.
Limited Competition in the Cardioprotection Market
Our analysis identified only one notable competitor to NYR in the cardioprotection market: Infensa Bioscience, an Australian biotechnology company. Infensa is developing a novel class of inhibitors derived from spider venom, designed to protect the heart and brain following stroke and myocardial infarction. These inhibitors function by blocking acid-sensing ion channel 1a (ASIC1a), a key driver of acid-induced cell death in both cardiac and neural tissues. Currently, Infensa remains in the preclinical stage of development.
The scarcity of competitors in the cardioprotection space underscores both the novelty and potential value of NYR’s lead candidate, Xolatryp. With few alternative treatment options in development, NYR is well-positioned to capitalise on this emerging market and establish a competitive advantage in addressing a critical unmet medical need.
NEUROPROTECTION PROGRAM
Program Overview – A Novel Mechanism of Action
Nyrada’s lead candidate for its Brain Injury Program, Xolatryp, is a Transient Receptor Potential Canonical (TRPC) ion channel blocker with a novel mechanism of action designed to provide neuroprotection for stroke and traumatic brain injury (TBI) patients.
TRPC channels, located in cell membranes, regulate non-selective positive ion flow, influencing neuronal excitability, neurotransmitter release, and gene expression. Overactivation of these channels during neuronal injury leads to calcium overload, a key factor in cell death and brain damage. By blocking TRPC channels, Xolatryp aims to prevent excessive calcium influx, protecting neurons and mitigating the severity of brain injury in stroke and TBI.
Preclinical Stroke Study
In early 2024, Nyrada commenced a preclinical study on Xolatryp to assess its effectiveness in preventing secondary brain injury after a stroke. The company announced on 28 February 2024 that the study demonstrated significant neuroprotection, with Xolatryp reducing secondary brain injury in the penumbra region by an average of 42% (p = 0.0213). The study, conducted in collaboration with UNSW Sydney, used a photothrombotic stroke model in test animals. Treatment with Xolatryp began 30 minutes post-injury and continued via intravenous infusion for 72 hours. MRI analysis confirmed the drug’s efficacy, with no adverse effects observed. Currently, no FDA-approved treatments exist for secondary brain injury, highlighting Xolatryp’s promising potential.
Good Laboratory Practice (GLP) Studies
Nyrada began Good Laboratory Practice (GLP) studies in March 2024 to assess the safety and toxicology of Xolatryp after the preclinical stroke study results in February 2024. The studies, involving rats and dogs, aimed to ensure reliable safety data for human trials. Eight studies were conducted, with results from the final study released on October 16 2024. By December 31 2024, Nyrada submitted its Phase I clinical trial regulatory package for review, and received approval from the Human Research Ethics Committee on February 7 2025.
Preclinical Walter Reed TBI Study
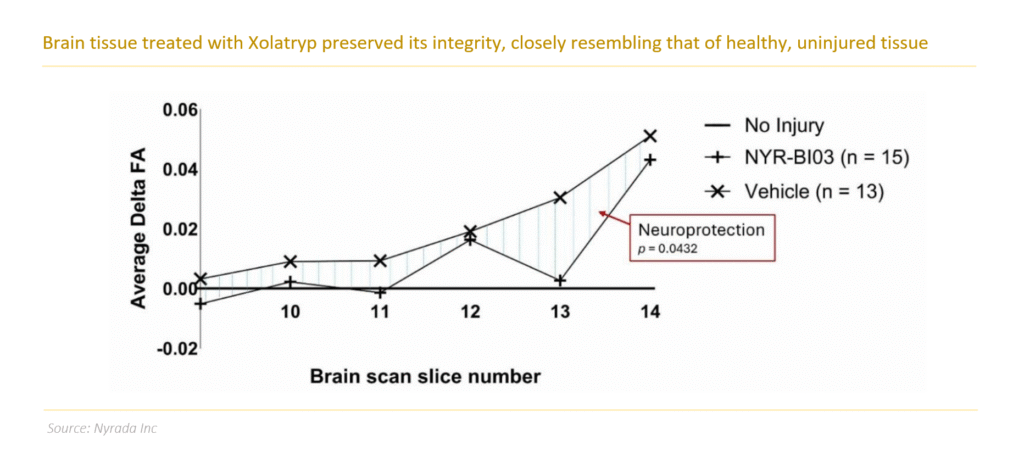
In 4Q FY24, NYR commenced a collaborative TBI study with the Walter Reed Army Institute of Research (WRAIR) and UNSW Sydney. The study evaluated the neuroprotective efficacy of Xolatryp in a preclinical model using WRAIR’s proprietary rodent model, designed to replicate severe head injuries experienced by military personnel. The study evaluated 28 test animals that received a continuous intravenous infusion of either Xolatryp or a vehicle control over 48 hours. In line with NYR’s previous preclinical stroke research, UNSW performed high-resolution magnetic resonance imaging (MRI) using its advanced small animal imaging facility to assess brain tissue integrity.
On 7 April 2025, NYR announced that its study demonstrated strong neuroprotective effects of Xolatryp in reducing secondary TBI. Using a validated WRAIR model, animals treated with Xolatryp showed statistically significant improvements (p = 0.043 via ANOVA) compared to those receiving a vehicle control. Advanced MRI analysis across six consecutive brain sections near the injury site revealed that the treated group maintained tissue integrity closer to that of uninjured brains. This was measured by comparing the deviation in fractional anisotropy (delta FA), with values closer to zero indicating less damage.
Neuroprotection Market Landscape Presents Significant First-Mover Advantage
The neuroprotection market is largely undeveloped, with no FDA-approved treatments for preventing secondary brain damage after TBI or stroke, presenting a major opportunity. Few companies are pursuing neuroprotective therapies, giving NYR a strong first-mover advantage. Competitors include Argenica Therapeutics (peptide therapy in Phase II), Astrocyte Pharmaceuticals (small-molecule therapy in Phase I), and Cellvation Inc (cellular therapy in preclinical stage). The limited competition and high unmet need position NYR to potentially lead in this emerging field.
CLINICAL TRIALS
Phase I Clinical Trial
Overview. The study, which commenced in March 2025, aims to evaluate the safety, tolerability, and pharmacokinetics of Xolatryp. The study is a randomised, placebo-controlled trial which initially comprised five cohorts, each consisting of eight healthy volunteers – six receiving the active drug and two receiving a placebo. Dosing began at low concentrations, with dosage levels gradually increasing in subsequent cohorts. Participants received an intravenous dose of Xolatryp or placebo over three hours, followed by a 48-hour monitoring period for safety assessments and pharmacokinetic blood sampling. NYR’s trial site operator, Scientia Clinical Research, managed participant recruitment.
Cohort Dosage. On 31 March 2025, NYR announced that all participants in its Phase I clinical trial had been dosed and discharged. Two sentinel participants were first dosed—one with Xolatryp, the other with a placebo—as a standard safety measure. After reviewing their safety data, the remaining participants were dosed. In total, six received Xolatryp and two received a placebo in this double-blind, randomised, placebo-controlled, dose-escalation study. All doses were administered via a three-hour infusion.
Clinical Trial Protocol Amendment. On 4 June 2025, following the successful dosing of cohort 3, NYR announced that it had received approval from the HREC to amend the Phase I clinical trial protocol. The modifications allowed the evaluation of a higher dosage and extended treatment duration, reflecting the strong safety and tolerability profile observed across all cohorts dosed thus far. As a result, the Phase I study was expanded to include six cohorts.
Completion of Dosage. On July 21, 2025, NYR announced the successful completion of dosing across all six cohorts in its ongoing clinical trial. Progress remained consistent throughout the study, with the Safety Review Committee (SRC) authorising advancement through each cohort following favourable safety and pharmacokinetic assessments. Notably, no safety signals, dose-limiting toxicities, or unexpected adverse events have been reported to date. A comprehensive safety and pharmacokinetic review will be conducted by the SRC once all data is available. All the data will then be analysed in preparation for the final clinical study report, expected in the coming months.
Strategic Refocus
Xolatryp has demonstrated strong preclinical efficacy across three key indications: stroke, TBI, and acute myocardial infarction (AMI). While academic studies suggest broader therapeutic potential, NYR has opted to concentrate its efforts on cardioprotection. This decision is driven by the robust preclinical cardiac data and the limited availability of non-dilutive funding for TBI in the U.S. Accordingly, the company will direct the majority of its financial and human resources toward advancing Xolatryp’s development in cardioprotection. Concurrently, Nyrada remains committed to progressing its stroke and TBI programs. The company will also continue to evaluate new pipeline opportunities and pursue non-dilutive funding avenues in Australia, the U.S., and other key markets.
Phase II Trial
Overview. With the Phase I trial of Xolatryp nearing completion, on 23 July 2025, NYR announced its commitment to a Phase IIa clinical trial. The Phase IIa trial design seeks to evaluate Xolatryp as a first-in-class intravenous therapy to limit heart muscle damage and prevent arrhythmias during ischemia and after reperfusion in patients with ST-Elevation Myocardial Infarction (STEMI) that undergo Percutaneous Coronary Intervention (PCI).
Study Design. NYR’s planned Phase IIa trial will enrol up to 150 STEMI patients in Australia to assess two dosage levels of Xolatryp, administered via infusion for up to six hours. The trial is expected to begin in Q1 2026, pending completion of the ongoing Phase I study and HREC approval. The primary endpoint is safety, with secondary endpoints focused on early signals of functional cardiac outcomes. These are supported by strong preclinical data, GLP-compliant safety and toxicology studies, and encouraging results from Nyrada’s near-complete Phase I trial in healthy volunteers. The company is currently finalising the Phase IIa design and will provide further details once cost estimates are confirmed.
MARKET OVERVIEW
Stroke Market
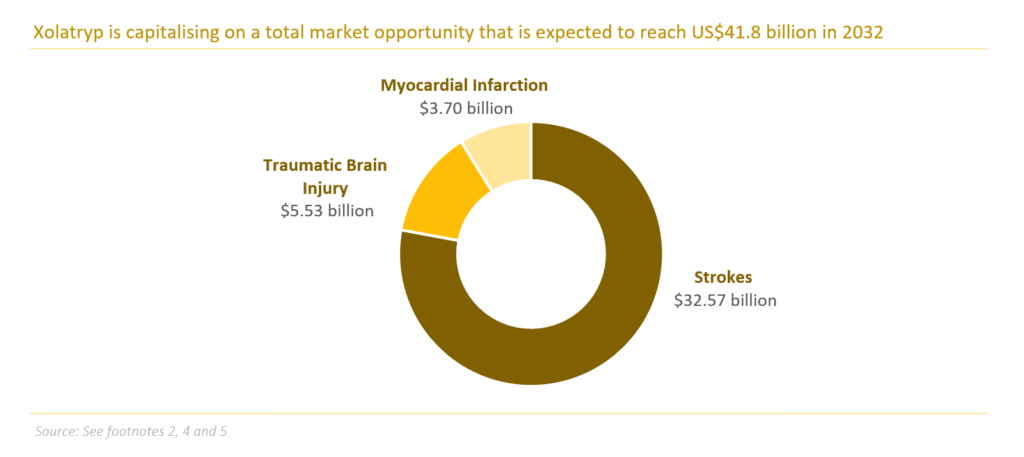
Each year, 15 million people worldwide experience a stroke, with 5 million losing their lives and another 5 million left permanently disabled, creating significant challenges for families and communities[1]. Despite the apparent need for effective treatments, there is only one approved drug class for stroke suitable for <15% of patients, which is tissue plasminogen activator (tPA). Driven by innovation in treatment options, the global stroke treatment market is expected to grow at a 7.5% CAGR to US$58.09 billion in 2031 from US$32.57 billion in 2023[2].
Traumatic Brain Injury Market
An estimated ~5.5 million people are suffering severe TBI annually, with ~55 million living with the effects of medically treated TBI[3]. It is clear that effective treatment can significantly enhance patient outcomes and lower the substantial costs linked to the long-term care of brain injury survivors. However, there is currently no FDA-approved treatment available on the market. Continued advancements in available treatments are expected to drive the growth of the global TBI treatment market from US$3.46 billion in 2022 to US$5.53 billion in 2030[4].
Myocardial Infarction Market
Globally, 15-20 million people suffer myocardial infarction annually, with a 15% mortality rate within 30 days[5]. Among survivors, 20-30%—particularly those experiencing cardiac arrest—develop acquired brain injury due to oxygen deprivation during arrest and reperfusion injury post-resuscitation. This leads to cognitive, neurological, or motor impairments, creating a significant unmet need. The market for myocardial infarction therapies, projected to reach US$3.7 billion by 2032, offers substantial growth potential. Xolatryp, targeting brain injury post-myocardial infarction, represents a transformative opportunity to address this gap, improve patient outcomes, and reduce long-term disability burdens.
[1] World Health Organisation – Stroke, Cerebrovascular accident
[2] Data Bridge Market Research – Global Stroke Market Size, Share, and Trends Analysis Report
[3] National Academies of Sciences, Engineering and Medicine – Traumatic Brain Injury
[4] Global Traumatic Brain Injuries Treatment Market – Industry Trends and Forecast to 2030
[5] Spherical Insights – Global Myocardial Infarction Market Size To Grow USD 3.7 Billion By 2032
KEY PEOPLE
-

John Moore
Non Executive Chairman
John Moore is an experienced executive with a diverse background in leadership roles across various industries. John’s prior experience includes serving as CEO of Acorn Energy from 2006 to 2015. During his tenure, the CoaLogix business was acquired for US$11m and later sold for US$101m. Additionally, the Comverge business was listed in the US before being sold to Constellation Energy. Prior to Acorn Energy, John was a Partner and CEO of Edson Moore Healthcare Ventures, where he oversaw the acquisition of sixteen drug delivery investments from Elan Pharmaceuticals for US$148m. John holds a Bachelor of Arts from Rutgers University in the US.
-

James Bonnar
CEO
James brings over 25 years of global experience in the Life Sciences industry, including preclinical research, clinical operations management, CMC (Chemistry, Manufacturing and Controls), Regulatory Affairs, and Quality Assurance. Before joining Nyrada, James was at Neuren for eleven years across various roles, including as the Director – Clinical Operations, where he oversaw clinical development for drugs in the areas of TBI and neurodevelopmental disorders. Prior to that, he worked in diabetes research, GMP manufacturing, and drug formulation development.
-

Benny Evison
Chief Scientific Officer
Benny brings to Nyrada expertise in advancing drug compounds from the discovery phase into clinical trials in humans. After earning a Bachelor of Medical Science with Honours and a PhD from La Trobe University, his doctoral research identified a novel mechanism of action for Pixantrone, a drug used to treat non-Hodgkin’s lymphoma. Seeking international experience, Benny became a postdoctoral fellow at St. Jude Children’s Research Hospital in Memphis, where his work on DNA repair-targeting drugs enhanced chemotherapy effectiveness. Inspired by his time with critically ill children, he returned to Australia as one of Nyrada’s founding scientists, driving impactful research and development.
-

Christopher Cox
Non Executive Director
Christopher Cox is a Co-Founder and Managing Partner of Population Health Partners since April 2020. He is also a Senior Attorney and retired Partner at Cadwalader, Wickersham & Taft LLP, where he led the Corporate Department and served on the Management Committee. With expertise in mergers and acquisitions, restructurings, spin-offs, and complex financing, Chris was seconded from 2016 to 2019 to The Medicines Company as Executive Vice President and Chief Corporate Development Officer, overseeing business development and strategy. Earlier in his career, he was a partner at Cahill Gordon & Reindel LLP. Currently, Chris is the CEO of Symphony Capital Holdings, LLC, a private investment firm with interests in biotechnology, network security, and entertainment.
-

Dr. Rüdiger Weseloh
Non-Executive Director
Rüdiger Weseloh is the Executive Director of Business Development at EMD Serono, Inc. in Rockland, MA, USA. Over his 18-year tenure, he has led more than 80 transactions for the healthcare division of its parent company, Merck KGaA, Darmstadt, Germany. His deal-making expertise spans the entire drug development value chain, with a focus on oncology, rheumatology, neurodegenerative diseases, and fertility. Prior to joining Merck KGaA, Rüdiger spent five years as a Biotech and Pharma Equity Analyst at Gontard & Metallbank AG in Frankfurt and Sal. Oppenheim in Cologne/Frankfurt. Earlier in his career, he conducted three years of postdoctoral research at the Max Planck Institute for Experimental Medicine in Göttingen. Additionally, he served for five years on the Supervisory Board of Cytotools AG in Freiburg, Germany.
-

Marcus Frampton
Non Executive Director
Marcus Frampton is the Chief Investment Officer of the Alaska Permanent Fund Corporation (APFC), a US$80 billion sovereign wealth fund for the State of Alaska. In this role, he oversees APFC’s investment team and leads all portfolio investment decisions within the strategic framework set by the Board of Trustees.
Frampton joined APFC in 2012, bringing a diverse background in investment banking, private equity, and asset management. He began his career as an Investment Banking Analyst and Associate at Lehman Brothers (2002–2005) before transitioning to private equity investing at PCG Capital Partners (2005–2010). He later served as an executive at LPL Financial, a private equity-backed portfolio company, from 2010 to 2012.
-

Dr Gisela Mautner
Non- Executive Director
Gisela Mauntner is a seasoned international business leader with extensive experience in pharmaceutical product development, corporate strategy, and commercial execution in competitive global markets. She currently serves as CEO and Managing Director of Noxopharm Ltd (ASX:NOX).
Throughout her career, Gisela has held senior roles at Amgen, Bayer, Siemens Medical Solutions, and Merck/MSD, driving both commercial and scientific success. She has a strong global network in the pharmaceutical industry and has held key leadership positions within the Australian Pharmaceutical Physicians Association (APPA, now MAPA), including President, Vice President, and Treasurer. She also represents Australia in the International Federation of Associations of Pharmaceutical Physicians (IFAPP).
-

Ian Dixon
Non Executive Director
Dr Dixon holds a PhD in biomedical engineering from Monash University and an MBA from Swinburne University. He brings extensive technical and entrepreneurial expertise in founding, scaling, and managing technology-driven companies, with a strong focus on the commercial potential and challenges of early-stage drug development. In 2011, he co-founded Cynata Inc., now a subsidiary of ASX-listed Cynata Therapeutics Ltd (ASX: CYP), which is advancing the Cymerus stem cell therapy for conditions such as osteoarthritis, ARDS, and critical limb ischemia.
GET INVESTMENT OPPORTUNITIES OR
RAISE CAPITAL
Contact Us
Access Canary Capital Research
Sign up to our mailing list to access our research reports.
By submitting your details, you agree to our Terms of Service.